The coronavirus pandemic has transformed so many things in our lives, from the way we work to the way we socialise. But the impact has not been experienced equally. While the whole of the UK population was asked to practice social distancing during the lockdown, one newly created category of people was asked to pay special care to reduce their own exposure to the disease: those who were identified as being at high risk from complications from COVID-19 (or SARS-CoV-2). These “clinically extremely vulnerable” people were asked to take action beyond normal social distancing to protect themselves from SARS-CoV-2.
In a letter received by many people who were defined as clinically extremely vulnerable, they were informed that:
“The safest course of action is for you to stay at home at all times and avoid all face-to-face contact for at least 12 weeks from today, except from carers and healthcare workers who you must see as part of your medical care.”
The impact of the creation of this category, through the establishment of the Shielded Persons List (SPL) by NHS Digital, cannot be understated. From the outset there have been questions around the effects that the shielding rules have had on the mental and physical wellbeing of people affected due to isolation, financial and practical difficulties.[1] In addition, the method of the list creation, application, communication and revision has also had major impacts on people. For many people who were, or were not, included on the SPL, and for many whose status changed, there has been confusion, uncertainty, mistrust, and feelings of vulnerability with regards to what actions they should take.
In our public involvement work many people who were shielding felt that they had to make decisions for themselves (or contact charities for advice) about whether they should be shielding.[2] This was often in the absence of support from their healthcare providers, whom they felt were busy with the COVID-19 response. The uptake of the guidance has varied substantially depending on how much individuals felt like they were appropriately categorised, and also whether they felt that the guidance matched their own risk perceptions. It has also meant that many people decided that they should have been included on the list and decided to shield themselves.
Part of this uncertainty about whether this category fits an individual was due to the way in which the list appears to be based in an automated algorithm, which feels impersonal or perhaps ill-suited when applied to an individual. Some of the uncertainty and mistrust can also be associated with the dynamic processes that underpin the list production. Unpacking these process helps to clarify why responses to this list have been so varied.
To create the SPL, NHS Digital first deployed expert clinicians to create a list of high-risk disease groups, and people were then assigned to the SPL if they had these conditions. Most people on the SPL were identified centrally through an algorithm that mapped the list of high-risk conditions onto individual level diagnosis categories. They “…‘translate’ (or map) the clinical requirements of the list into the right subsets of coded information so that individual patients could be identified.” Additional people were added to the SLP by GPs and through secondary care following clinical guidance. The list is maintained centrally, but flows out to clinicians through local data systems, and can be updated by primary and secondary clinicians at the point of care. Any updates are then taken into the national list on a weekly basis, which is then distributed the following week through the same channels.
This sounds organised, and in some ways makes intuitive sense: there are diseases and conditions that suggest people are likely to have worse reactions to COVID-19, so there is a national list created of people with these conditions using rules (an algorithm) created by experts to map conditions onto continually collected data.
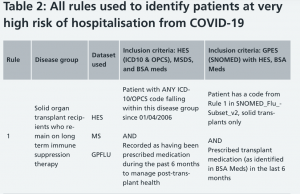
An example of a rule used to map a condition to datasets (https://digital.nhs.uk/coronavirus/shielded-patient-list/methodology/)
After the initial list was created, clinical decision making by doctors who know the patients’ histories can override the algorithm. In one interview about how the algorithm works in practice, a GP said
“The data – it gives you the false sense of precision because a code is a code…., but actually on a human level, there is something else going on. And the data will help us and it may be a very rough way to screen people, but somebody has to do another level of tailoring to the patient, to the individual.”
The same doctor said that they will also defer to the advice of a charity as to whether to add a flag to include a patient on the list. How a person finds out they are on the SPL is determined entirely by who adds them to the list, because responsibility to inform them lies with the person or body that adds the SPL flag to their file. They can be informed by their GP, through secondary care, or NHS Digital. The dynamic nature of the list production, including the tailoring for the patient at the local level, has meant that the process can appear chaotic and impersonal to people who are affected. The list, which is partially a product of their own health data, becomes unrecognisable as it is transformed and recontextualised for use in the COVID-19 era.
A predictive risk algorithm is being developed in Oxford University [3] that extends the current SPL list. It will build on the category of “clinically extremely vulnerable” people with a prediction about how you will respond if you get COVID-19. This prediction will be based on the responses of people with similar clinical and demographic backgrounds who have now had COVID-19. The idea that underpins this algorithm is that people who have data that is statistically similar to yours (people like you) will have similar responses to COVID-19.
The algorithm as described by the research protocol (Oxford University):
The original SPL… was developed early in the outbreak when there were very little data or evidence about the groups most at risk of poor COVID-19 outcomes, and so was intended to be a dynamic list that would adapt as our knowledge of the disease improved and more evidence became apparent… [we will] assess whether a predictive risk algorithm can be developed with the above evidence to permit a more sophisticated ‘risk stratification’ approach. There are a variety of potential uses for such a tool, but it is primarily anticipated that it could be used both clinically in informing patients of their individual risk category and managing them accordingly, and strategically to stratify the population for policy purposes.[4]
In our research at Imperial, some people have said that they would much prefer an individualised risk assessment, but it remains to be seen whether this new form of algorithmic personalisation will feel more appropriate than the current SPL category production process.
On August 1st, shielding was paused in England, Scotland and Northern Ireland, and it was paused on August 16th in Wales. The pause in shielding has meant that many people have lost the protection and support that were provided because they were on the SPL, and those on the shielding list are no longer eligible for Statutory Sick Pay. Furthermore, the application of shielding guidance can now also be adjusted at the local level according to local data on prevalence. If there is an increase in prevalence, people on the list may be told that they now need to shield. The list itself remains very much alive and may be reactivated as the situation evolves. As SARS-CoV-2 transmission increases over the coming weeks, people who are considered vulnerable are likely to receive further communications about their risk, and it will be crucial to see whether the more approach feels any more personal.
[1] Robb CE, de Jager CA, Ahmadi-Abhari S, Giannakopoulou P, Udeh-Momoh C, McKeand J, Price G, Car J, Majeed A, Ward H, Middleton L. Impact of social isolation on anxiety and depression during the early COVID-19 pandemic: a survey of older adults in London, UK. Frontiers in Psychiatry 2020;11:591120 doi: 10.3389/fpsyt.2020.591120
[2] Maria Piggin, Katherine Collet, Philippa Pristerà. Insight Report: Guidance for people who are clinically extremely vulnerable from COVID-19 (18 June 2020)
[3] Hippisley-Cox et al. 2020. “Development and evaluation of a tool for predicting risk of short-term adverse outcomes due to COVID-19 in the general UK population.” Research Protocol
[4] Hippisley-Cox et al. 2020. “Development and evaluation of a tool for predicting risk of short-term adverse outcomes due to COVID-19 in the general UK population.” Research Protocol